About Lehe
乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。


乐于心,和与众,与己乐,与人和; 心宽念纯,百病无生。


If pancreatic cancer is considered as “the king of cancers” due to its “extremely high malignancy”, “rapid progression”, and “short survival time”.
The fact that liver cancer can be ranked among the “three major cancer kings”“difficult to treat” is certainly related to its
“
difficulty.
According to statistics, the recurrence rate of liver cancer is high. After surgical resection of liver cancer, the 3year recurrence rate can be as high as 50%, and the 5year overall recurrence rate reaches 50% to 70%. Patients with recurrence have a very poor prognosis, and the 5year survival rate may only be 30% to 40%[1-2].
Overview of the illness
One year after surgery, there was a recurrence for the second time. Is it just bad luck?
In January 2015, Mr. Yan felt discomfort in his upper abdomen for two consecutive days and underwent an abdominal CT scan. The scan revealed a low-density mass lesion in the lower segment of the right lobe of the liver, measuring approximately 6.1*6.2*6.9cm. After enhancement, the lesion showed rapid enhancement and rapid washout, suggesting a tumor lesion.
A tumor the size of an egg?!
Mr. Yan promptly sought medical attention and underwent a "laparoscopic resection of the right posterior liver segment (including parts of segments Ⅴ, Ⅵ, Ⅶ, and Ⅷ) +cholecystectomy" on
the 26th day of January 2015. Postoperative pathology revealed: (right liver) poorly differentiated hepatocellular carcinoma .
At this time, Mr. Yan thought the surgery had ended with the removal of the tumor, unaware that the risk of recurrence had already been lurking.
Unlike benign tumors, malignant tumors often have some cancer cells that have spread to other tissues and organs before surgery, creating opportunities for subsequent recurrence.
Previous studies have found that more than 50% of patients with liver cancer have already experienced dissemination and metastasis of cancer cells at the time of initial diagnosis. The overall recurrence rate after radical resection for liver cancer is 5years, reaching 50% to 70%. Even for small hepatocellular carcinoma (early-stage liver cancer), the postoperative recurrence rate can be around 40%. The main reason is related to the dissemination and metastasis of malignant tumors.
In addition, Mr. Yan's liver cancer is a low-differentiated hepatocellular carcinoma. For primary liver cancer, especially hepatocellular carcinoma, tumors often grow on the basis of chronic liver disease and cirrhosis. Sometimes, even if the primary lesion is removed, the original “unhealthy soil” can still grow new lesions, which is known as “multicentric occurrence”.
The facts also confirm the "difficulty" of liver cancer. In April 2015, on the 28th day of the month, Mr. Yan underwent a postoperative follow-up MRI examination of the upper abdomen. The MRI results showed postoperative changes in the right liver, with a small nodule measuring 0.7cm in size in the third segment of the liver. It is considered to be a recurrence of liver cancer. AFP:211.5ng/ml ↑.
2015 Year5Month7On [date] (month) [date] (day), the patient underwent "laparoscopic left liver cancer resection" and the postoperative pathology revealed a moderately differentiated hepatocellular carcinoma of the left liver.
In 2015 (year) 9 (month) 7 (day), a follow-up MRI was performed, which showed a small nodule in segment V of the liver. EBO-MRI indicated recurrence of liver cancer. AFP: 155.3ng/ml↑
In 2015 (year) 9 (month) 18 (day), the patient underwent "laparoscopic right liver recurrent liver cancer resection" and the postoperative pathology revealed a moderately differentiated hepatocellular carcinoma of the liver.
Since the diagnosis of liver cancer, the cancer has recurred 8 months, with 2 recurrences and 3 surgeries. These disseminated metastatic cancer cells cannot be removed by surgery and can only wait for recurrence --to be resected --and then recur --to be resected again?
Immunotherapy, as the fourth major therapy for cancer treatment, has given Mr.Yannew hope for long-term tumor control. Professor Zhang Minghui's Lehe New Medical Team found after evaluating Mr. Yan's condition that:< H243>
1、 Mr. YanWhen the tumor was first removed, the tumor was relatively large and effective adjuvant therapy was not given to improve the patient's prognosis after surgery. Recurrence is a high probability event.
2、 Postoperative adjuvant drug therapy (targeted therapy, chemotherapy (transarterial chemoembolization)< H302>transcatheter arterial chemoembolization,TACE) As well as immune modulator therapy, drug resistance has become an unavoidable issue in this treatment method, and its applicability and safety also need to be further evaluated. It is not an ideal postoperative adjuvant therapy.
3、vNKT Cellular immunotherapy, as a leader in killing tumor cells,vNKTImmune cell transfusion is a systemic treatment.Whether it is residual cancer cells that have not been completely cleared by surgery or cancer cells that have spread and metastasized through, systemic treatment is more thorough..
In addition,vNKTCell immunotherapycan directly kill cancer cells,andregulate the immune microenvironment inside tumor tissue, killing inhibitory immune cellsMDSCsBreaking the immune escape of tumors, rebuilding the normal immune system, and providing multi-channel protection for preventing recurrence and metastasis.

Natural killer T (NKT) cells are a special T-cell subset that possess both T-cell receptor (TCR) and NK cell receptors on their surface. They combine the important characteristics of NK cells and T cells, with the dual ability to recognize tumor cells both nonspecifically and specifically, and can rapidly kill tumor cells. Among the NKT cell subsets, there is a larger and more potent special type of NKT cell, discovered by the experimental team led by Professor Zhang Minghui at Tsinghua University, known as vNKT (Variant Natural Killer T) cells.
The number of these vNKT cells in the body is very small, and they are not easily activated. However, once activated, they can single-handedly eliminate those tumor cells that may remain undetected in the body. In addition, research has also found that vNKT cells have dual anti-tumor effects. Not only can they directly kill cancer cells, but they can also regulate the immune microenvironment within tumor tissues, kill inhibitory immune cells known as myeloid-derived suppressor cells (MDSCs), break tumor immune evasion, rebuild the normal immune system, and further prevent recurrence and metastasis.
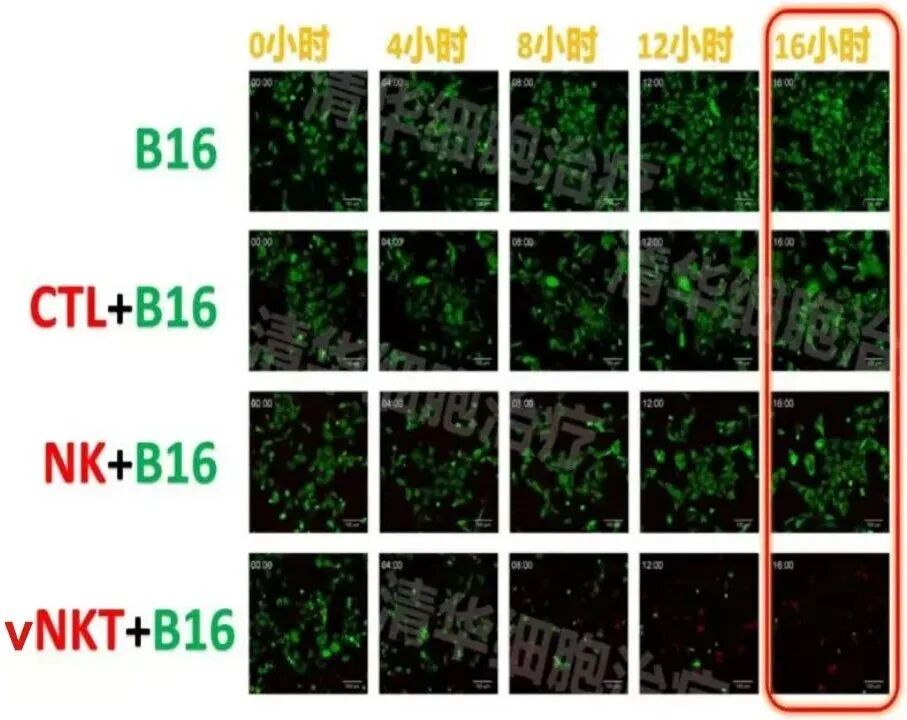
Experimental conditions: In the presence of vNKT cells, nearly all B16 tumor cells were killed after 16 hours!
After detailed comparison, evaluation, and communication of treatment options, in 2015, Mr. Yan began to undergo 11months of vNKT cellular immunotherapy. By 2024, Mr. Yan had completed 39treatment courses, and his condition has remained stable for 9years with follow-up. Mr. Yan's mental state has also been free from anxiety, with good appetite and sleep. No signs of recurrence or metastasis were found during follow-up examinations, and the "difficult to treat" curse of liver cancer has finally been broken.
Conclusion and Review< H624>
The postoperative period of cancer surgery is a critical time for preventing recurrence and metastasis, especially for patients with tumors that are highly malignant and have a high risk of recurrence. Scientific management is necessary to more thoroughly eliminate cancer cells.
It is not difficult to see Mr. Yan's case. There is no suitable follow-up treatment after surgery, which leads to the inability to guarantee the continuity of treatment, resulting in ineffective removal of residual cancer cells and disseminated cancer cells, leaving room for recurrence and metastasis.
Special attention should be paid to high-risk groups: late tumor staging (III-IVstage), frequent lymph node metastasis, poor pathological differentiation (such as undifferentiated cancer, poorly differentiated cancer), postoperative residual lesions or genetic testing indicating high recurrence risk (such asTP53mutations).
Primary liver cancer is currently the fourth most common malignant tumor and the second leading cause of cancer-related deaths in China, posing a serious threat to the lives and health of our people. Due to the insidious onset of liver cancer, less than 30% of patients are suitable for radical treatment at the time of initial diagnosis. Systemic anti-tumor therapy plays a crucial role in the treatment of advanced liver cancer. Immunotherapy, represented by targeted and immune checkpoint inhibitors, plays a significant role in the treatment of advanced liver cancer. However, patients often experience progression after second-line treatment, and there is a lack of corresponding guidelines or consensus for medication or treatment guidance, putting clinicians and patients in a difficult situation regarding medication.
In addition to immune checkpoint inhibitors, immunotherapy for malignant tumors also includes active immunotherapy that activates the body's autoimmune function. Among these, NKT cells are of particular interest due to their dual characteristics of both NK and T cells. Activated vNKT cells (variant NKT) can not only directly kill tumor cells but also kill myeloid-derived suppressor cells in the tumor microenvironment (TME), thus potentially offering better tumor treatment effects.
vNKT immunotherapy for hepatocellular carcinoma brings new hope to patients with advanced liver cancer who have progressed after second-line treatment. To this end, Professor Zhang Minghui's Lehe New Medical Research Team at Tsinghua University and Shanghai East Hepatobiliary Surgery Hospital have jointly launched a clinical research recruitment program for patients with advanced hepatocellular carcinoma, aiming to benefit more patients who meet the clinical research criteria!
How to participate?
If you are a liver cancer patient or a family member, you can contact our assistant to provide your patient's medical records. After a one-on-one assessment of the condition by a professional medical team, you can apply to participate in the clinical research. For details, please scan the QR code for consultation

Scan QR Code
Communicate with Professor Zhang Minghui's Team
Liver Cancer Patient Exchange Group Professor Zhang Minghui of Tsinghua University has always harbored the great wish of "a world without disease" and is committed to providing a patient-centered platform for patients to exchange and help each other. Whether you are newly diagnosed, troubled by side effects, unsure how to choose a treatment plan, want to exchange experiences and insights, or simply pour out your heart, you are welcome here!
There are professional experts giving lectures and enthusiastic group members communicating in the group, and there are also opportunities to apply for clinical research enrollment. Join the group and live a happy and healthy life!

Founder of Lehe New Medical
Professor Zhang Minghui, who holds a PhD in Immunology from Tsinghua University School of Medicine, has led a research team for over 20 years since the discovery of vNKT cells in 2002. They have accumulated treatment experience in over 700 cases of solid tumors, covering almost all common solid tumors. The research results fully demonstrate the great value of vNKT cells in the treatment of solid tumors.

It is suitable for patients with high pathological malignancy or a risk of recurrence after surgery; patients whose tumors have been basically controlled but not cured through conventional treatments such as chemotherapy, radiotherapy, and targeted therapy; patients with persistent high carcinogenic factors; and patients who are intolerant to radiotherapy and chemotherapy. If these patients do not receive effective follow-up treatment after traditional anti-tumor therapy, recurrence, metastasis, or reoccurrence of tumors will be highly probable. In this case, vNKT cell therapy is an ideal follow-up treatment method that can significantly improve patient prognosis.
[1]Guidelines for Liver Cancer Screening in Chinese Population (2022, Beijing)
[2] CHOI J, JO C, LIM YS. Tenofovir versus entecavir on recurrence of hepatitis B virus-related hepatocellular carcinoma after surgical resection[J]. Hepatology, 2021, 73(2): 661-673. DOI: 10.1002/hep.3128
Click on the image to view past issues and exciting content


Address: Room 1101 (Unit 101), 11th Floor, Building 1, No. 7 Courtyard, Kexueyuan Road, Life Science Park, Changping District, Beijing
Phone:010-8265 9866
Email:lehemedneo@hotmail.com